- Monday - Friday 8:30-4:30pm [Closed for lunch Noon to 12:30-1:30pm]
- 1200 N. Federal Hwy, Suite 100, Boca Raton, FL 33432
You know something is wrong – but you don’t know what it is – but it scares you.
That feeling of strangeness in your chest may very well be palpitations. And we know exactly how to diagnose it, and how to treat it as well. That is our specialty.
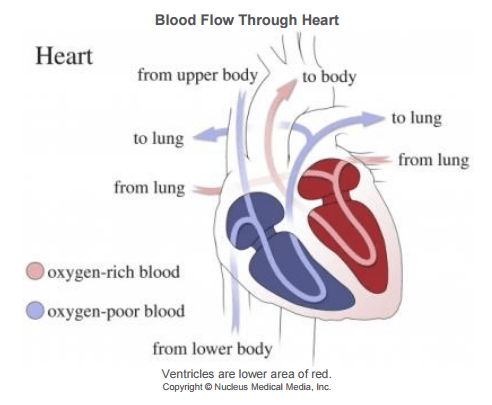
The heart, as you know, is a type of organic machine. It draws blood (which carries nutrients and oxygen) from the lungs, to the body, and having delivered it’s load of sustenance, brings it back to the lungs, to once again reinvigorate and redeliver it’s precious cargo.
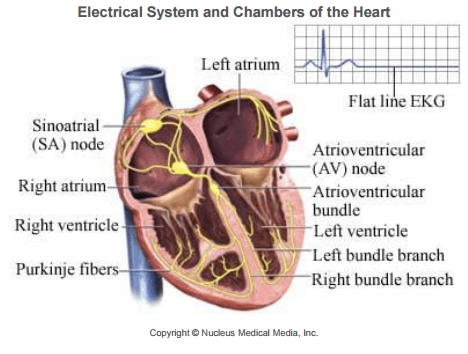
What you may not know, is that in addition to being this incredible “blood pump”, the heart is controlled by electrical pulses. And that’s where we come into your life picture.
We have been practicing this established corridor of medicine for over 20 years. We have specialized treatment rooms at the Boca Raton Regional Hospital and at the Delray Medical Center.
We can bring your palpitations under control and often cure them for life.
We want to assist you in regaining your lifestyle as it once was.
We can do it. Call us, We want to help.
Atrial fibrillation is an abnormal heart rhythm. The heart’s electrical system normally sends regularly spaced signals.
These signals tell the heart muscle to contract or beat.
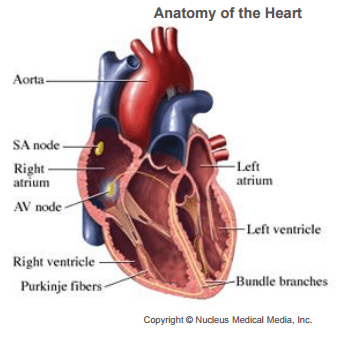
The heart has two upper chambers called atria. It also has two lower chambers called ventricles. Each signal starts in the atria and travels to the rest of the heart. The electrical signals from the atria are fast and irregular when you have atrial fibrillation. The atria shake instead of contract. Some signals do not reach the ventricles and the ventricles continue pumping. This pumping is usually irregular and sometimes rapid. This rhythm can reduce the heart’s ability
to pump blood out to the body.
Blood left in the heart chambers can form clots. These clots may sometimes break away and travel to the brain. This can cause stroke.
Here at Cardiac Arrhythmia Service we have a structured approach to deal with atrial fibrillation. We may recommend a cardioversion, medications or an ablation procedure. We are highly experienced and have successfully performed over 1,000 ablations.
What happens during AFib?
Normally, your heart contracts and relaxes to a regular beat. In atrial fibrillation, the upper chambers of the heart (the atria) beat irregularly (quiver) instead of beating effectively to move blood into the ventricles.
If a clot breaks off, enters the bloodstream and lodges in an artery leading to the brain, a stroke results. About 15–20 percent of people who have strokes have this heart arrhythmia. This clot risk is why patients with this condition are put on blood thinners. Even though untreated atrial fibrillation doubles the risk of heart-related deaths and is associated with a 5-fold increased risk for stroke, many patients are unaware that AFib is a serious condition.
According to the 2009 “Out of Sync” survey:
Only 33% of AF patients think atrial fibrillation is a serious condition
Less than half of AF patients believe they have an increased risk for stroke or heart-related hospitalizations or death
AFib Treatment Saves Lives & Lowers Risks
If you or someone you love has atrial fibrillation, learn more about what AFib is, why treatment can save lives, and what you can do to reach your goals, lower your risks and live a healthy life.
If you think you may have atrial fibrillation, here are your most important steps:
Know the Atrial fibrillation (also called AFib or AF) is a quivering or irregular heartbeat (arrhythmia) that can lead to blood clots, stroke, heart failure and other heart-related complications. At least 6.1 million Americans are living with AFib.
Here’s how patients have described their experience:
What happens during AFib?
atrial fibrillationNormally, your heart contracts and relaxes to a regular beat. In atrial fibrillation, the upper chambers of the heart (the atria) beat irregularly (quiver) instead of beating effectively to move blood into the ventricles.
If a clot breaks off, enters the bloodstream and lodges in an artery leading to the brain, a stroke results. About 15–20 percent of people who have strokes have this heart arrhythmia. This clot risk is why patients with this condition are put on blood thinners.
Even though untreated atrial fibrillation doubles the risk of heart-related deaths and is associated with a 5-fold increased risk for stroke, many patients are unaware that AFib is a serious condition.
Excerpted from the American Heart Association
Definition
Atrial fibrillation is an abnormal heart rhythm. The heart’s electrical system normally sends regularly spaced signals.
These signals tell the heart muscle to contract or beat.
The heart has two upper chambers called atria. It also has two lower chambers called ventricles. Each signal starts in the atria and travels to the rest of the heart. The electrical signals from the atria are fast and irregular when you have atrial fibrillation.
The atria shake instead of contract. Some signals do not reach the ventricles and the ventricles continue pumping. This pumping is usually irregular and sometimes rapid. This rhythm can reduce the heart’s ability to pump blood out to the body.
Blood left in the heart chambers can form clots. These clots may sometimes break away and travel to the brain. This can cause stroke.
Sudden Arrhythmia Death Syndromes (SADS) are genetic heart conditions that can cause sudden death in young, apparently healthy, people. These conditions can be treated and deaths can be prevented.
Warning Signs of SADS
SADS conditions occur because the electrical system of the heart is not working properly, so that the heart beats with an abnormal rhythm.
Facts about SADS Conditions
Each year in the United States, 350,000 Americans die suddenly and unexpectedly due to cardiac arrhythmias. Almost 4,000 of them are young people under age 35. (CDC 2002)
Please click here if you or a child you know have any of these Warning Signs
Because SADS condition are passed down from parent to child, each child of an affected parent has a 50% chance of inheriting the condition. It is estimated that over half of the 4,000 SADS deaths each year of children, teens, or young adults have one of the top two warning signs: 1) family history – of a SADS diagnosis or sudden unexplained death (usually undiagnosed and untreated) of a family member, or 2) fainting.
1 in 200,000 high school athletes in the US will die suddenly, most without any prior symptoms—JAMA 1996; 276
Excerpt from the SADS Foundation
Definition
The heart has four chambers. It has two upper chambers (atria) and two lower chambers (ventricles). Electrical signals regulate the heart beat. The signals also help the atria and ventricles work together in the same rhythm. The blood from the atria is pushed into the ventricles and leave the heart to circulate to the rest of the body. Atrial flutter is a type of abnormal fast beating ( arrhythmia) in the atria. These fast beats make it difficult for the atria to pushing all the blood into the ventricles. As a result, the ventricles push less blood through the body.
Atrial flutter may be an acute or chronic disorder that comes and goes. Atrial flutter is not usually life-threatening when it is treated. However, it may increase your risk of developing blood clots and stroke.
This condition can be treated. Contact your doctor if you think you may have atrial flutter.
Wouldn’t it be great to have a full time team of doctors, nurses and medical assistants accompanying you everywhere you go?
They could check your heart rhythms 24/7 – even when you sleep. And then, if they noticed something gone awry, wouldn’t it be great to get immediate service? A mild shock to put your heart back into perfect sinus rhythm. The way it’s supposed to be.
No – this is not science fiction. It’s the reality of implantable devices.
We are experts in clinically evaluating your exact needs, and then taking care of them. In certain instances, it might be necessary to “implant” an electrical monitor, just under the surface of your skin.
Every year doctors implant over 133,262 defibrillators.
It’s a common and successful procedure, and allows us here at Cardiac Arrhythmia Service to continually monitor the condition of your heart.
For pacemakers or defibrillators
Risks of procedure are mainly infection – if that occurs, the entire system must be removed, injury to the lung requiring placement of a chest tube for 1-2 days, injury to the heart muscle or lead dislodgement requiring repositioning. The risk of any of these is less than 1 percent.
These are palpitations and they are often caused by an abnormal heartbeat.
We are experts at finding the etiology of the palpitations and potentially curing it. We want to help you regain your lifestyle back.
Be sure to check the menu item MORE for printable files about Pre-op Information.
We, like you, have witnessed the hundreds of miracles of the modern age.
Google, Facebook. Email, on-line shopping, movies on-demand, and lately, Self Driving Cars.
But these incredible advances in our everyday lives have impacted medicine in much the same ways.
In the mid 1800’s, Luigi Galvani an electrical scientist and experimenter demonstrated the effect of electricity on living beings. He administered an electric shock to dead frogs, and the frogs legs twitched. So it has been well documented that electricity is a large part of the human make-up for nearly two hundred years.
But it wasn’t until August 1958 when Seymour Furman introduced a pacemaker rhythm device into a human heart to help adjust heart sinus rhythm. It was an unwieldy affair (compared to today), needing external power. But only months later, at the University of Minnesota, a transistorized, battery powered version of the same concept was introduced, and modern Electrophysiology was born.
Today we can installed mobile devices like pacemakers, defibrillators and loop monitors, in a standardized manner; safely, quickly and dependably.
Several devices can be utilized to detect arrhythmia in order to make the diagnosis or to assess the frequency and duration of arrhythmia
Monitoring of pacemakers and defibrillators is utilized to detect predictable and unpredictable arrhythmias as well as device hardware problems.
SVT is a rapid heart beat arising from the top chambers of the heart. There are several causes of SVT. SVT often arises from an extra circuits in the heart which is present at birth and is activated later in life. The most common circuit is in the middle of the hearts electrical system next to AV node called dual AV nodes and AVNRT (The AV node electrically joins the top chambers called atria and bottom chambers called ventricles). Extra circuits joining the top and bottom chambers of the heart may also be present on the right or left side of the heart (WPW). Finally the source can be a single focus coming from the right or left top chamber of the heart (atrial tachycardia).
The diagnosis is usually made by electrocardiogram or event monitor during an episode of SVT. To stop an acute episode vagal maneuvers such as bearing down can help. In the long termthe treatment for SVT is usually medication or an ablation. While medications can sometimes reduce the severity of the episodes they do no eliminate the extra. An ablation is a relatively low risk procedure that eliminates the extra circuit and cures the problem.
For pacemakers or defibrillators
Risks of procedure are mainly infection – if that occurs, the entire system must be removed, injury to the lung requiring placement of a chest tube for 1-2 days, injury to the heart muscle or lead dislodgement requiring repositioning. The risk of any of these is less than 1 percent.
The risk of SVT ablation or VT ablation is injury to a vein in the groin which can require local surgery, injury to the heart muscle or ending up needing a pacemaker. The risk of any of these is well below 1 percent.
Been passing out a lot lately?
Well you are not alone.
Syncope is a sudden loss of consciousness. There are many causes of syncope but the most common cause is vasovagal or neurocardiogenic syncope. This occurs to patients who have no structural heart disease and is rather a blood pressure regulation problem. Other causes of syncope include a sudden change of heart rhythm either fast or slow or other medical causes.
Been passing out a lot lately?
Well you are not alone.
Syncope is a sudden loss of consciousness. There are many causes of syncope but the most common cause is vasovagal or neurocardiogenic syncope. This occurs to patients who have no structural heart disease and is rather a blood pressure regulation problem. Other causes of syncope include a sudden change of heart rhythm either fast or slow or other medical causes.
Although it seems that people faint for no reason, there are often specific triggers that cause SYNCOPE. It may be as simple as standing for a long time in a hot environment, or the sight or sensation of a needle (taking or giving blood). It is also not uncommon for emotional stress to trigger SYNCOPE, but there are also occasions where there still apparently seems to be no cause.
Often in syncope, the sufferer will experience prodromal (warning) symptoms such as nausea (feeling sick), sweating, light-headedness or going pale. These symptoms correlate with increased vagal tone (increased signal in the vagus nerve supplying the heart), which acts to momentarily slow the heart and/or dilate (widen) the blood vessels in the body, leading to a reduction in blood flow to the brain (cerebral perfusion). This in turn leads to a loss of consciousness as the brain becomes starved of oxygen.
On suffering syncope, the subject will then often fall to the floor. This then allows blood to reach the brain again as the effect of gravity is negated and results in a rapid regaining of consciousness. Rapid recovery is one of the hallmark features of SYNCOPE can help distinguish it from some more sinister causes.
Another cause of syncope can be an arrhythmia – a fast, slow or irregular heart beat. By not pumping blood effectively, there is a decrease in blood and oxygen supplied to the brain which can cause loss of consciousness. If we suspect that an arrhythmia may be the etiology of syncope we will recommend cardiac monitoring to help establish a diagnosis.
There are many causes for syncope and it essential to make an accurate diagnosis so that we can treat the underlying problem and prevent a recurrent episode of syncope. If you or anyone you know suffers from this problem please come see us so we can diagnose the problem, treat the underlying cause and prevent future episodes
Definition
Tachycardia is a rapid heart rate of more than 100 beats per minute. Sinus tachycardia, from the heart’s sinus node,
is a normal response to exercise, illness, or stress.
There are several types of abnormal tachycardias or arrhythmias.
These can come from two places:
This condition can be life-threatening. But, it can be treated. If you think you or someone you know has this condition,
get emergency help.
SYNCOPE AND A TILT-TABLE TEST
There are many causes of fainting, losing consciousness or having lightheaded spells. In most cases, the situation can be diagnosed by a cardiac electrophysiologist. When people have syncope, i.e. a sudden loss of consciousness, if they have a history of heart problems such as a previous heart attack or wear heart muscle (cardiomyopathy), there is a high suspicion that the cause of the syncope was rapid, dangerous rhythm disturbance called “ventricular tachycardia.”
This determined further by an EP (electrophsiologic) study.
Most people who have syncope, however, have no cardiac history and have normal hearts. The most common cause of their syncope is called “neurocardiogenic” or “vasovagal” syncope. This problem in itself is not dangerous. The only danger lies in a situation, i.e. in the wrong place and wrong time. The best test to determine if this is the cause of syncope is called a tilt-table test.
When one experiences neurocardiogenic syncope, we believe that the following is the body’s response and so-called mechanism: When a person stands up or sits up, blood pools into the veins in the legs by gravity. In some people, the return of blood to the heart is slower than normal, and at the time the heart responds by pumping blood a little more forcefully. This is also a normal response, but in those who suffer from neurocardiogenic syncope, this response is exaggerated and the heart pumps a lot stronger. This triggers pressure receptors inside the heart which tell the brain that the pressure inside the heart is too high. This is, of course, a false message. The brain then overreacts, as well, and both opens up the arteries by withdrawing all of its adrenalin-type activity and tells the heart to slow its heart rate down, which is an outflow of the nervous system which slows and calms the body system. This, in turn, takes a normal blood pressure and drops it suddenly to a very low blood pressure. Not enough blood and oxygen gets to the brain, the patient faints, and when one falls to the ground blood returns to the heart and everything is restored.
Often before losing consciousness patients receive a warming that something may happen. This warning may last a few seconds or minutes. Typically people report feeling hot or sweaty, claustrophobic, short of breath, lightheaded, or nauseated. After passing out and coming to, the patient often feels unwell and tired for some time thereafter.
The tilt-table test tries to provoke the problem. Ideally one would have had an episode of syncope in front of a doctor; however, since that is not usually possible, we try to bring it on in front of us. The test is usually done in the morning, on an empty stomach. An intravenous line is inserted, a blood pressure cuff is applied, and heart rhythm is continuously monitored. The patient lies on a bed and is strapped to the bed for safety reasons. The bed is simply tilted to an almost upright position, i.e., 70 to 80° leaning back only slightly, and the patient stands there for up to 25 minutes. We do not have the patient swinging in various angels and upside down. After 15 minutes, if nothing occurs, usually for another ten minutes and we continue to monitor heart rate and blood pressure. Once the patient reports feeling faint and blood pressure drops, the test
will be terminated. The table is returned back to the lying position, and the patient feels better usually within a dew minutes. We sometimes do provoke loss of consciousness, which can be uncomfortable.
There is no risk involved in this test, i.e. no risk of anything more dangerous happening than the fainting itself. Because the patient is strapped to the table, there is not risk of injury/ this may, however, cause the same comfortable feeling as the patient experienced outside at home. In some situations, a repeat test on medication is advised to ensure that the syncope will not recur.
Allow one hour for the test. You may leave after the test, but we advise that someone else drive you as you may feel unwell after the test. The results are known immediately and reported to you and whoever is with you immediately. We then contact your doctor within 24 hours. There are various medications to try for this problem. Not all are immediately successful and it does involve a trial-and-error basis. Please ask your doctor for any other questions.
Definition
The ventricles are the large lower chamber of the heart. They are responsible for moving blood to the organs and tissues of the body. In ventricular fibrillation, the heart’s ventricles contract in a rapid and chaotic manner. As a result, little or no blood is pumped from the heart. Unless medical help is provided immediately, ventricular fibrillation will lead to cardiovascular collapse and sudden death.
Definition
Ventricular tachycardia is an abnormally fast heart rate. The abnormal heart rate originates in one of the heart’s lower chambers (ventricles). It is diagnosed when there are three or more beats in succession originating from a ventricle. The heart beats at a rate greater than 100 beats per minute, but less than 200 beats per minute. Ventricular tachycardia is considered sustained if it lasts more than 30 seconds. When this condition is sustained, the ventricles are not able to fill with enough blood for the heart to keep blood flowing properly through the body. This can result in lowered blood pressure, heart failure, and death.
Ventricular tachycardia is a fast heart rate that arises from improper electrical activity in the lower chambers or ventricles of the heart. If there is no structural heart disease, it is usually not life threatening and can be treated with ablation or medication.
If there is structural heart disease such as coronary artery disease, heart attack in the past, Weak heart or a genetic abnormality, VT may rapidly generate into ventricular fibrillation and become fatal within a few seconds. When people die suddenly it is usually from ventricular tachycardia or ventricular fibrillation . The more dangerous forms of ventricular tachycardia are treated with a defibrillator, medications, ablation or a combination of the above.
Although a few seconds may not result in problems, longer periods are dangerous. Short periods may occur without symptoms or present with lightheadedness, palpitations, or chest pain. Ventricular tachycardia may result in cardiac arrest and turn into ventricular fibrillation. Ventricular tachycardia is found initially in about 7% of people in cardiac arrest.
Ventricular tachycardia can occur due to coronary heart disease, aortic stenosis, cardiomyopathy, electrolyte problems, or a heart attack. Diagnosis is by an electrocardiogram (ECG) showing a rate of greater than 120 bpm and at least three wide QRS complexes in a row. It is classified as non-sustained versus sustained based on whether or not it lasts less than or more than 30 seconds. The term “ventricular tachycardias” refers to the group of irregular heartbeats that includes ventricular tachycardia, ventricular fibrillation, and torsades de pointes.
In those who have a normal blood pressure and strong pulse, the antiarrhythmic medication procainamide may be used. Otherwise immediate cardioversion is recommended. In those in cardiac arrest due to ventricular tachycardia cardiopulmonary resuscitation (CPR) and defibrillation is recommended. Biphasic defibrillation may be better than monophasic. While waiting for a defibrillator, a precordial thump may be attempted in those on a heart monitor who are seen to go into an unstable ventricular tachycardia. In those with cardiac arrest due to ventricular tachycardia survival is about 45%. An implantable cardiac defibrillator or medications such as calcium channel blockers or amiodarone may be used to prevent recurrence.
Extracted from Wikipedia
For pacemakers or defibrillators
Risks of procedure are mainly infection – if that occurs, the entire system must be removed, injury to the lung requiring placement of a chest tube for 1-2 days, injury to the heart muscle or lead dislodgement requiring repositioning. The risk of any of these is less than 1 percent.
The risk of SVT ablation or VT ablation is injury to a vein in the groin which can require local surgery, injury to the heart muscle or ending up needing a pacemaker. The risk of any of these is well below 1 percent.


Courtesy of the American Academy of Physician Assistants:
What is a physician assistant?
A physician assistant (PA) is a medical professional who works as part of a team with a doctor. A PA is a graduate of an accredited PA educational program who is nationally certified and state-licensed to practice medicine with the supervision of a physician.
What can PAs do?
PAs perform physical examinations, diagnose and treat illnesses, order and interpret lab tests, perform procedures, assist in surgery, provide patient education and counseling and make rounds in hospitals and nursing homes. All 50 states and the District of Columbia allow PAs to practice and prescribe medications.
How are PAs educated and trained?
The PA educational program is modeled on the medical school curriculum, a combination of classroom and clinical instruction. The PA course of study is rigorous and intense. The average length of a PA education program is 27 months.
Admission to PA school is highly competitive. Applicants to PA programs must complete at least two years of college courses in basic science and behavioral science as prerequisites to PA school, analogous to premedical studies required of medical students. The majority of PA programs have the following prerequisites: chemistry, physiology, anatomy, microbiology and biology. Additionally, most PA programs require or prefer that applicants have prior healthcare experience.
PA education includes instruction in core sciences: anatomy, physiology, biochemistry, pharmacology, physical diagnosis, pathophysiology, microbiology, clinical laboratory science, behavioral science and medical ethics.
PAs also complete more than 2,000 hours of clinical rotations, with an emphasis on primary care in ambulatory clinics, physician offices and acute or long-term care facilities. Rotations include family medicine, internal medicine, obstetrics and gynecology, pediatrics, general surgery, emergency medicine and psychiatry.
Practicing PAs participate in lifelong learning. In order to maintain national certification, a PA must complete 100 hours of continuing medical education every two years.
There are currently 170 accredited PA programs in the United States. The vast majority award master’s degrees. PA education programs are represented by the Physician Assistant Education Association and accredited through the Accreditation Review Commission on Education for the Physician Assistant (ARC-PA).
How do doctors and PAs work together?
By design, physicians and PAs work together as a team, and all PAs practice medicine with physician supervision. Supervision does not mean, though, that a supervising physician must always be present with the PA or direct every aspect of PA-provided care.
PAs are trained and educated similarly to physicians, and therefore share similar diagnostic and therapeutic reasoning. Physician-PA practice can be described as delegated autonomy. Physicians delegate duties to PAs, and within those range of duties, PAs use autonomous decision-making for patient care. This team model is an efficient way to provide high-quality medical care. In rural areas, the PA may be the only healthcare provider on-site, collaborating with a physician elsewhere through telecommunication.
PAs deliver high-quality care, and research shows that patients are just as satisfied with PA-provided care as they are with physician care.
This will close in 0 seconds
This will close in 0 seconds
This will close in 0 seconds
This will close in 0 seconds
This will close in 0 seconds
This will close in 20 seconds
This will close in 20 seconds
This will close in 20 seconds
This will close in 20 seconds
This will close in 20 seconds
This will close in 20 seconds